
In June 2020, in accordance with the 21st Century Cures Act of 2016 and the Prescription Drug User Fee Act (PDUFA), the U.S. Food and Drug Administration (FDA) launched Project Patient Voice. This patient-focused drug development initiative facilitates systematic approaches to collecting and using meaningful patient and caregiver input, to better inform medical product development and regulatory decision-making, taking the use of real-world evidence (RWE) to a new level.
As big data continues to transform and innovate the U.S. healthcare system, RWE remains a credible source for scientific inquiry. However, the evolving dynamics of the healthcare environment, including COVID-19’s impact, is creating a growing problem. Payers are now pushing for value-demonstrating evidence, which is shaping the types of evidence generation required by various stakeholders in the healthcare ecosystem as their focus shifts to value and outcomes. The problem is these new levels of complexity are bringing with them knowledge gaps as the industry lacks in sophisticated evidence requirements.
Today, the industry focuses on high volumes of data, causing an uneven quality of de-identified real-world data (RWD), as quality is sacrificed for quantity. These massive data sets are then analyzed in fragmented organizational and technological silos, forcing decision makers to rely on poor-quality analysis with limited transparency as they do not have the ability to validate the actual source of the data.
Fortunately, this massive problem brings with it tremendous opportunity, as RWE is the powerful disruptor we need to unlock a new and deeper level of transparency, not only for better understanding the disease area and treatments, but to drive increased connectivity and outcomes between pharma, healthcare providers (HCP), payers, and patients.
We must remember why we began collecting RWD in the first place: to bring better value and outcomes to patients. If we simply focus on what we are doing — amassing large quantities of datasets — we lose sight of the “why” and fail to meet the demands of today’s market. The FDA’s commitment to a more patient-focused drug development process makes it clear it is time to stop focusing on the “what” and create a new, convergent model that meets the needs of today’s “why.”

Ramita Tandon
Chief Operating Officer
Trio Health
A New Engine for a New Era
To truly crack the code and get the most value we can from RWE, we need to combine the qualitative insights from the patient voice and the quantitative clinical evidence into an integrated, evidence management engine. This is key to offering high-quality insights into the patient’s journey, like their reasons for choosing, switching, and discontinuing therapies.
This engine needs to employ a robust, linked data infrastructure that effectively syncs and analyzes the qualitative and quantitative data in real-time, while also including direct access to the HCP and patient, allowing for validation and supplementation of RWD as needed. The blueprint of this engine must also include a governance body to review and manage the risk from the various RWE activities.
This approach moves us out of the old models of gathering disparate and siloed RWD, and into a framework that pushes the envelope by taking a more holistic and deeper approach. It is only through using quality datasets from a verified feedback loop that we can unlock the patient journey and optimize the HCP and patient experiences along with outcomes.
The Rheumatology Engine
Leading the Way
At Trio Health, we already built and tested this engine in the rheumatology community. Rheumatoid arthritis (RA) is a complex, chronic disease commonly treated with high-cost specialty medications. Trio Health and the American Rheumatology Network (ARN), a national network of large community practices, initiated a partnership in 2019 with the goal of improving patient outcomes.
With data from more than 369,000 patients serviced by ARN, the goal was to understand the rate of therapy changes, patients’ reasons for change, the associated symptoms, and ultimately the impact on both patient-reported and clinically measured outcomes.
To gather the complete picture of care, Trio Health designed a multidimensional platform with nightly collection of fielded data (e.g. labs, prescriptions, disease assessments, infusions, medical claims) and open text elements (e.g. patient comments and concerns, physician natural language assessments) from electronic medical records. This platform not only extracts transactional data, but also serves as a central hub for supplementation and source verification, allowing communication with HCPs and patients when more information is required.
An independent, multi-disciplinary steering committee that includes key opinion leaders from ARN, former senior FDA officials, and RWE experts, serves as the governance structure to oversee the data engine, ensuring credibility, trust, and transparency. This system provides an unprecedented level of high-quality assurances for regulatory-grade accuracy.
Higher Quality Data Means Higher Quality Insights
Through this platform, Trio Health analyzed the rate of therapy switching and found:
- 25% of the patients could be considered “well tolerated and effective” who remained with a giventherapy for prolonged periods (multi-year).
- 33% of patients could be considered “well tolerated but not effective” in that their switching pattern was more aligned with expected failure rates.
- The remaining patients (~40%) were aligned with “impulsive-poorly tolerated but largely effective.”
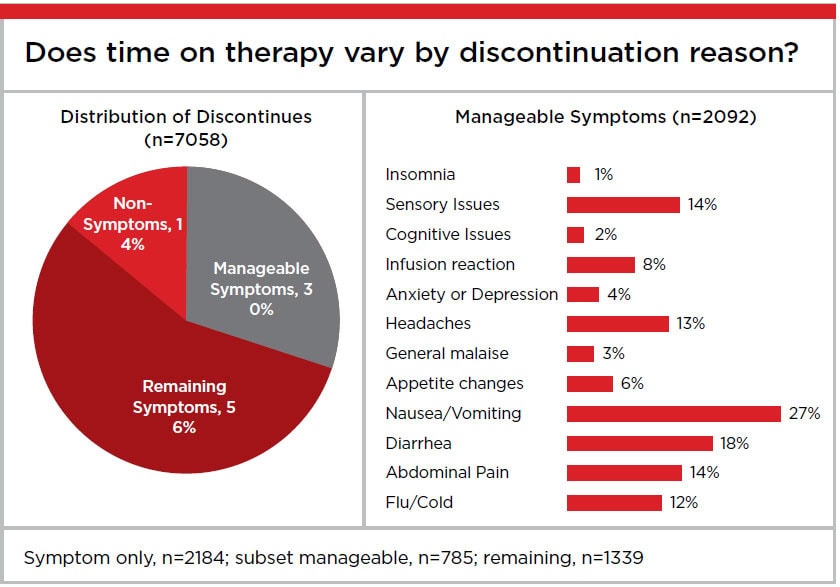
To better understand the many factors that influence a decision to change therapy, Trio Health specifically assessed the impact of clinical, operational, financial, and subjective influences from stakeholders on treatment discontinuation. Among the multiple factors that drive discontinuations, the key findings were:
- Symptoms were associated with the majority (>85%) of discontinuations.
- A third of discontinuations due to symptoms were manageable symptoms (e.g. nausea, headaches, cold symptoms).
- The patient voice drove discontinuation in half of all cases.
The reason for discontinuation was directly related to time on therapy. Patients who discontinued treatment due to manageable symptoms did so three times faster than those who discontinued due to other reasons. The tragedy of medication discontinuation due to manageable symptoms is that providers are unlikely to retry a medication once it has been abandoned, significantly limiting the patient’s future options. As such, maximizing the therapeutic benefit of each treatment is in the interest of all.
These findings mean we can improve patient outcomes by communicating with HCPs to inform decisions around common discontinuation reasons. Meaningful interventions, such as addressing the manageable symptoms without discontinuing the medication, can then be deployed at the point of care, maximizing therapeutic benefits. This creates an incredibly
valuable feedback loop never seen before.
To go one step further to assess at a disease level with no bias, Trio Health built a large symptomatic Patient Voice database
(>100,000 patients) that carefully categorizes symptoms, life events, and lack of efficacy for each discontinued regimen. To determine the catalyst for the switch, Trio Health investigated the relative impact of the patient voice as well as the provider-performed clinical assessment to determine lack of efficacy) at the time of discontinuation.
The investigation further underscored the need to combine the reasons why patients switch or discontinue therapy with historical trends and other influences that may be impacting such actions.
The Difference Between Model-T and Tesla Engines
Comparing the lessons from our rheumatology evidence management engine to today’s standard, fragmented data collection, is like comparing a Model-T engine to a Tesla. They are completely different machines. We built an engine that runs on an entirely new source of fuel: quality, verified, and synced data from both qualitative and quantitative sources. This new way of marrying quantitative data with qualitative patient voice not only improves the HCP-patient interaction, it opens up the opportunity to solve problems we could not see before.
These new insights bring solvable problems to light, enabling decision makers to immediately deploy tailored actions across the product’s lifecycle, further supporting the FDA’s commitment to patient-centered drug development. It’s a continuous feedback and improvement loop that is already spurring collaboration across stakeholders (patients, payers, HCPs, pharma), inspiring the creation of educational programs at the point of care, informing clinical trial designs and regulatory decisions, plus increasing payments that support reimbursement strategies.
Fueling Future Engines
The next step in fueling more of these engines is to build a blueprint for curating and linking data at the highest quality level for all disease areas. Our insights reveal that the patient voice, largely through symptom complaints, is highly impactful on medication switching, which is why it is in the best interest of all that we create engines for every disease area.
It is imperative we make these changes before the next COVID-19 catches the industry off-guard. We need to put the infrastructure in place now so we are ideally positioned to develop and deploy focused interventions that support providers in better understanding data trends and intervening to maximize therapeutic benefits to patients when the next disease
crisis arises.
The tools are already at our fingertips, we simply need to reject the current status quo of accepting low-quality datasets and refocus on our “why”: our commitment to solutions that truly align the best interests of the patient and each stakeholder to achieve the highest clinical and commercial excellence possible.